Platelet Disorders and Genetic Vaccines Might Have A Biological Link, but It’s Negligible
Understanding the nature of the potential harm helps us discern its risk.
![]()
Following
20210406 Apr 6 · 10 min read
While this article might fuel vaccine hesitancy in some, I hope it will mainly get dispelled instead. In a word, a possible biological explanation for how genetic (mRNA/DNA) vaccines might trigger platelet disorders every once in a blue moon has been proposed. Platelet is a blood component that clots blood in blood vessels.
This article will delve into the specifics and can be heavy to read, so if you have to skim through it, please at least read the last section.
Genetic vaccines and platelet disorders
Genetic vaccines[i] include the
1. mRNA vaccine from Pfizer-BioNTech and Moderna, as well as the
2. DNA vaccine from Oxford/AstraZeneca (Ox/AZ).
Unlike traditional vaccines — such as the whole-microbe or protein subunit ones — that don’t enter cells, genetic vaccines rely on gene delivery into cells. The gene (mRNA or DNA) then instructs the cell to make proteins of a pathogen — such as the spike proteins of SARS-CoV-2 — to train the immune system. While the mRNA vaccines use lipid nanoparticles (LNPs), the DNA vaccine uses harmless adenovirus for gene delivery into cells.
1. DNA vaccine
As of 31 March 2021, the European Medicine Agencies (EMA) has recorded 62 cases of
1. cerebral venous sinus thrombosis (CVST) associated with
2. thrombocytopenia (low platelets)
among the 9.2 million doses of Ox/AZ vaccine given. Of the 62 cases, 44 happened in Europe and 14 resulted in death, with a pattern of affecting younger females.
Although the rate of 6.7 CVST cases per million is slightly higher than what we would expect in the general population — i.e., 5 cases per 1 million each year — it’s crucial to note that CVST may have been underdiagnosed before the pandemic.
As a result, several countries —namely, Germany, Sweden, France, and Canada — have restricted the Ox/AZ vaccine to the older populations only. On the other hand, Denmark and Norway completely restricted the use of the Ox/AZ vaccine. But the EMA has stated that there’s no evidence to support such restrictions.
Today [20210406], however, Marco Cavaleri, head of vaccines strategy at the EMA, stated that there might be a causal link: “It is becoming more and more difficult to affirm that there isn’t a cause-and-effect relationship between AstraZeneca vaccines and the very rare cases of blood clots associated with a low level of platelets.” The EMA is now looking into this matter.
2. mRNA vaccine
A commentary in the Journal of Hematology described 20 cases of immune thrombocytopenia (ITP) — where the immune system attacks the platelets — occurring within days among the >20 million people who received the Pfizer-BioNTech or Moderna mRNA vaccines in the U.S as of 2 February 2021.
Notably, 17 of those cases had no pre-existing ITP. But the commentary estimated that 17 cases per 1–2 weeks translate to 39,000 to 78,000 cases per year, similar to the baseline ITP incidence in the U.S. at 50,000 cases per year. Although many were hospitalized from these ITP incidents, only one death in New York has been recorded.
Still, the commentary authors cautioned, “We cannot exclude the possibility that the Pfizer and Moderna vaccines have the potential to trigger de novo [new] ITP (including clinically undiagnosed cases), albeit very rarely.”
Image from the author.

A possible biological explanation
Goh Kiang-Hua, MD, a consultant general surgeon and Fellow of the Royal College of Surgeons (FRCS), has previously hypothesized how mRNA vaccine might trigger ITP in rare instances. This point was mentioned in a previous article, titled “Concerns of Lipid Nanoparticle Carrying mRNA Vaccine into the Brain: What to Make of It?” [Also here.]
A text excerpt is provided here:
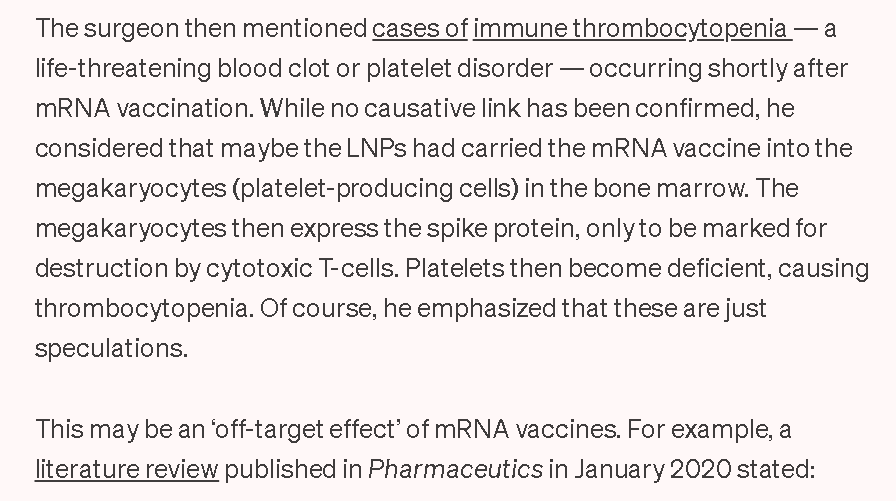
Image from the author. Abbreviation: LNPs: lipid nanoparticles that deliver the mRNA into cells.
The surgeon, Dr. Goh, informed me of the theoretical possibility of LNPs carrying mRNA vaccines into megakaryocytes in an email on 16 February 2021. He also speculated that “The vector vaccines [e.g., Ox/AZ] should be subjected to the same concerns.”
He recently referred me to response articles appearing in the British Medical Journal (BMJ) on 11 March 2021 that further shed light on how genetic vaccines might trigger platelet disorders every once in a blue moon. It started with a letter to the editor from Hamid A. Merchant, Ph.D., a subject leader at the Department of Pharmacy of the University of Huddersfield in England.
Dr. Merchant introduced that other viruses— such as the influenza virus, human immunodeficiency virus (HIV), and Dengue virus — can infect the platelets and megakaryocytes (platelet-producing cells). These infected cells may then be marked as foreign and destroyed by the immune system. Evidence also exists that SARS-CoV-2 could bind to the ACE2 receptor on platelets to promote blood clot disorders in Covid-19.
Dr. Merchant speculates that something similar might happen with genetic vaccines, writing that:
It is, therefore, not unreasonable to hypothesise that the genetic CoViD vaccines may also directly infect platelets and megakaryocytes triggering mRNA translation and consequent spike protein synthesis intracellularly. This may lead to autoimmune response against platelets and megakaryocytes… that may clinically manifest in thrombocytopenia, haemorrhage, and blood clots.
One notably subtlety is that, unlike megakaryocytes owning multiple nuclei (plural of nucleus), platelets do not have a nucleus that directs protein synthesis. But Dr. Merchant clarified that “Platelets are anucleate cells that continue to defy conventional logic; they are involved in mRNA translation and known to synthesise proteins for over fifty years.”
But DNA vaccine works by delivering the DNA into the cell nucleus to get transcribed into mRNA and then translated to proteins (see figure). So, this means that DNA vaccines won’t work in platelets that have no nucleus. As Paolo Gresele, MD, Ph.D., a professor of internal medicine, wrote in a rebuttal letter to Dr. Merchant: “Platelets although possessing a transcriptome and protein synthesis ability, are anuclear and can not transcribe genetic DNA information into mRNA.”
Dr. Merchant agreed on this point in another response article to Prof. Gresele. But Dr. Merchant added that mRNA vaccines, which bypass the cell nucleus to get translated into proteins, can still work in platelets, in theory (see figure).
Megakaryocytes, on the other hand, have many nuclei. So, DNA and mRNA vaccines are theoretically translatable into proteins in megakaryocytes, Dr. Merchant emphasized. The resulting immune attack at megakaryocytes might render the body unable to renew its platelets that need frequent renewal every 8–10 days, causing thrombocytopenia.
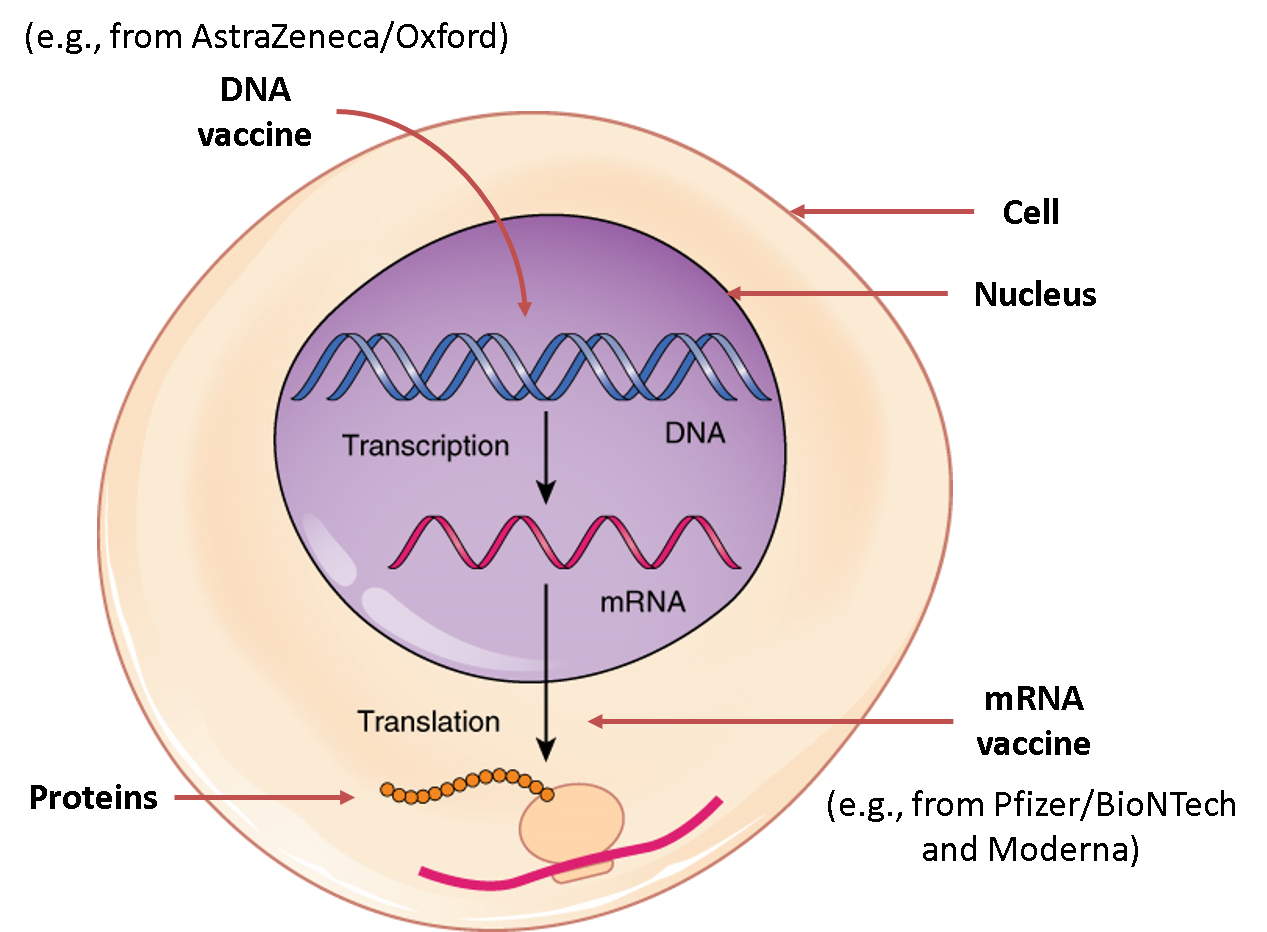
Figure adapted from Additional Biology. A simplified overview of how genetic vaccines get translated into proteins inside a cell. The DNA vaccine must first enter the nucleus to get transcribed into mRNA, which is then translated into proteins. But the mRNA vaccine can be directly translated into proteins without the nucleus.
Extra: Another possible biological explanation
Dr. Merchant has also speculated that the antibodies produced via vaccination might have become auto-reactive in rare situations. In fact, auto-reactive antibodies targeting the platelets have been detected in Covid-19 patients who developed blood clotting disorders.
So, it’s possible that antibodies generated against the spike proteins — be it via vaccination or real viral infection — might attack the platelets.
“Recently, scientists from Oslo [in Norway] identified an antibody from vaccinated individuals which they suspect being responsible for attacking platelets and causing recent thrombotic events,” Dr. Merchant clarified. “This discovery also supports our hypothesis that CoViD genetic vaccines may have a direct role in spurring autoimmune response against platelets that may clinically manifest in thrombocytopenia, haemorrhage, and blood clots.
Researchers from German have also claimed evidence of auto-reactive antibodies against platelets — called heparin platelet factor 4 — that caused the excessive blood clots and CVST following the Ox/AZ vaccine injection.
But the German and Norwegian data are not released or formally published, so we should regard them as preliminary and inconclusive for now.
The biodistribution of genetic vaccines
Although the safety and efficacy of genetic vaccines are well documented in clinical trials, the research on the tissue biodistribution — i.e., where the biomaterial ended up inside the body — of genetic vaccines is scarce.
Such biodistribution data isn't of utmost importance for the Food and Drug Administration (FDA) vaccine approval process. After all, in the final analysis, safety is the priority, and efficacy comes second.
1. mRNA vaccine
The European Medicines Agency (EMA) report of the Moderna mRNA vaccine has mentioned that “Low levels of mRNA could be detected in all examined tissues except the kidney” in rats. While the report did not state it explicitly, the bone marrow where megakaryocytes reside is presumably one of the examined tissues.
A 2017 mice study has also found that the influenza mRNA vaccine could enter the bone marrow in tiny amounts at 3.35 ng/mL. But this pales in comparison to that found in the muscle injection site, proximal lymph nodes, distal lymph nodes, and spleen at 5680, 2120, 177, and 87 ng/mL.
For the Pfizer/BioNTech mRNA vaccine, the Medicines & Healthcare products Regulatory Agency (MHRA) assessment report stated that “Information regarding the potential distribution of the test articles to sites other than the injection site following IM [intramuscular] administration has been provided and is under review as part of the ongoing rolling assessment.”
Such broad biodistribution of the mRNA vaccines can be attributed to the LNP technology, as discussed thoroughly here:
Concerns of Lipid Nanoparticle Carrying mRNA Vaccine into the Brain: What to Make of It?
Detailing the arguments for and against this concern with input from experts.
2. DNA vaccine
Dr. Merchant argued that “each dose of the vaccine contains a very high viral load (e.g., 50 billion viral particles/dose in Ox/AZ CoViD-19 vaccine and 100 billion viral particles/dose in Sputnik-V).” Sputnik-V is another DNA vaccine similar to the Ox/AZ’s one that uses harmless adenovirus for gene delivery.
“The viral particles are unlikely to be confined to the muscles at the injection site; they are free to distribute across the body and drain through lymphatic system; their apparent volume of distribution is likely to be very high,” Dr. Merchant continued.
He then cited the EMA’s report on the biodistribution of the Ox/AZ vaccine in mice. After 24 hours of intramuscular injection, “Although the highest levels of viral vector were observed in the injection site, low levels of distribution to some samples of all tissues were also observed,” the EMA report stated.
Studied tissues were “whole blood, injection site (skeletal muscle), brain, heart, draining inguinal lymph node, kidney, liver, lung, gonads, and spleen.” Bone marrow wasn’t included, unfortunately. But the EMA report further mentioned that another similar biodistribution study that involves the bone marrow is now on-going.
Closing remarks
So, all things considered, a possible biological explanation for the estimated 1–7 cases of platelet disorders from a million doses of genetic vaccines given might be due to its off-target effects in the bone marrow, megakaryocytes, or platelets that occur by a blind chance.
Ultimately, this article is mainly hypothetical. Thus far, there’s no concrete evidence proving that genetic vaccines could enter the megakaryocytes or platelets and then induce them to make the spike proteins of SARS-CoV-2.
Even if the platelets or megakaryocytes managed to create the spike proteins at the influence of genetic vaccines, we still don’t know the extent of damage it would cause.
If only tiny amounts of genetic vaccines — as shown in the 2017 mice study reviewed above — ended up in the bone marrow, perhaps only a few megakaryocytes would take up the genetic vaccine and make the spike proteins. If only a few megakaryocytes (or platelets) get destroyed by the immune system, this might be minor cellular stress that‘s harmless.
Still, it may be wise to be careful, especially in those susceptible to platelet disorders. As Dr. Merchant cautioned, “Genetic vaccines are new, and their long-term safety evaluation is a key to identify potentially contraindicated group of subjects, for instance patients with history of blood disorders, past or current thrombocytopenia or pre-existing immunological conditions.” This group of subjects might include those who mounted auto-reactive antibodies against the platelets following vaccination with the Ox/AZ DNA vaccine in Germany and Norway, as discussed above.
But even if this is true — that this group of individuals is at increased risk of platelet disorders from genetic vaccines — they are still incredibly rare. Recall that only <7 cases of ITP or CVST per a million genetic vaccine doses administered have happened thus far.
We should not forget that Covid-19 kills by attacking the respiratory and vascular (blood vessels) system. So, the risk of platelet or blood clotting disorders from Covid-19 (disease) or SARS-CoV-2 (virus) is real that has taken numerous lives, unlike the speculative risk from genetic vaccines.
Lastly, as mentioned, this article is mainly theoretical or hypothetical. Some might then wonder what’s the point of this article if everything isn’t confirmed. But I think that’s the point — to understand the hypothesis and why it’s just a hypothesis, and why the risk is negligible even if the hypothesis turned out to be true.